Akari Therapeutics Announces Positive Phase II Clinical Data in Orphan Blistering Skin Disease Bullous Pemphigoid at the 28th EADV Congress
- Treatment with nomacopan in six patients in Phase II trial was well tolerated and resulted in rapid onset of clinical improvement in five of six patients
– No reported drug-related serious adverse events
– Achieved marked reduction in Bullous Pemphigoid Disease Area Index (BPDAI) activity score and blistering
- Potential as monotherapy with the additional potential benefit of reducing steroid use which has multiple adverse effects in this frail population
° Two patients who received nomacopan monotherapy performed as well as those on a combined initial low-dose topical steroid plus nomacopan - Akari intends to present this new Phase II data to the
U.S. Food and Drug Administration (FDA) and theEuropean Medicines Agency (EMA) to advance its potential pivotal trial design for patients with BP - Nomacopan recently granted orphan drug designation by the FDA for the treatment of BP
NEW YORK and LONDON,
| |||||
BP is a severe orphan autoimmune inflammatory blistering skin disease with no approved treatments in the U.S. and Europe. The disease is primarily treated with steroids and immunosuppressants which bring with them well known side effects and an approximately three-fold increase in mortality in the elderly BP patient population.
“The positive safety profile and rapid response to treatment with nomacopan, even with no steroid co-medication, supports a treatment strategy that could see steroid use rapidly reduced in BP patients,” commented Clive Richardson, Chief Executive Officer of Akari Therapeutics. “As a result of this encouraging data, we now plan to develop our pivotal study design in conjunction with the FDA and EMA. We intend to begin the pivotal study in H2 2020, positioning nomacopan as potentially a first-in-class treatment for this severe and debilitating disease.”
In patients with BP there is evidence that both terminal complement activation (via complement component C5) and the lipid mediator leukotriene B4 (LTB4) have a central role in driving the disease. Ex vivo data in BP patients, recently published in the
The Phase II trial, which includes up to nine mild-to-moderate bullous pemphigoid patients, is a six-week (42 days of nomacopan dosing) open-label single-arm study evaluating safety and efficacy. Patients entering the trial were typically on the topical steroid mometasone which was stopped by day 21. The main efficacy measure is the Bullous Pemphigoid Disease Area Index (BPDAI) which along with blistering is a frequently used evaluation of the extent and severity of this skin disease.
Results showed that nomacopan, dosed daily subcutaneously, was well tolerated in six elderly patients (>55 years), and that there were no reported drug-related serious adverse events. This safety profile mirrors over 20 cumulative patient-years of data from patients treated with nomacopan across four other conditions in clinical development where no drug-related serious adverse events have been observed.
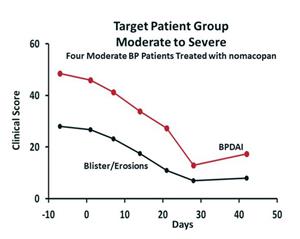
Four of the six patients were classified as at the upper limit of moderate BP. Moderate to severe patients represent about two-thirds of BP patients and are likely to benefit most from the potential to reduce or avoid steroids. These patients, who showed only a minor improvement on mometasone prior to initiation on nomacopan, saw a mean 41% and 63% decline in BPDAI score at day 21 and 42, respectively, and a 59% and 68% decline in blister score at day 21 and 42, respectively (see graph below of four moderate patients). One of the moderate patients had a flare up post day-28, which is not an uncommon on treatment as BP is a recurrent autoimmune disease.
Of the two mild patients, one patient showed a 100% decline in blisters by Day 21, sustained to day 42, and a decline in BPDAI score of 55% and 45% by day 21 and day 42, respectively. The other patient showed no response either on nomacopan or when switched to rescue steroids at day 28. This patient entered the trial after disease relapse while on steroid treatment.
Three of the patients who responded received mometasone steroids tapered to zero by day 21. Two other patients were on nomacopan only, with no steroids, and showed a similar beneficial response with a mean 39% and 79% drop in BPDAI activity at day 21 and day 42, respectively, and a 57% and 93% drop in blisters at day 21 and 42, respectively.
Dr. Christian Sadik, lead investigator from the
About Akari Therapeutics
Akari is a biopharmaceutical company focused on developing inhibitors of acute and chronic inflammation, specifically for the treatment of rare and orphan diseases, in particular those where the complement (C5) or leukotriene (LTB4) systems, or both complement and leukotrienes together, play a primary role in disease progression. Akari's lead drug candidate, Nomacopan (Coversin), is a C5 complement inhibitor that also independently and specifically inhibits leukotriene B4 (LTB4) activity. Nomacopan (Coversin) is currently being clinically evaluated in four indications: bullous pemphigoid (BP), atopic keratoconjunctivitis (AKC), thrombotic microangiopathy, or TMA, and paroxysmal nocturnal hemoglobinuria (PNH). Akari believes that the dual action of Nomacopan (Coversin) on both C5 and LTB4 may be beneficial in AKC and BP. Akari is also developing other tick derived proteins, including longer acting versions.
Cautionary Note Regarding Forward-Looking Statements
Certain statements in this press release constitute “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995. These forward-looking statements reflect our current views about our plans, intentions, expectations, strategies and prospects, which are based on the information currently available to us and on assumptions we have made. Although we believe that our plans, intentions, expectations, strategies and prospects as reflected in or suggested by those forward-looking statements are reasonable, we can give no assurance that the plans, intentions, expectations or strategies will be attained or achieved. Furthermore, actual results may differ materially from those described in the forward-looking statements and will be affected by a variety of risks and factors that are beyond our control. Such risks and uncertainties for our company include, but are not limited to: needs for additional capital to fund our operations, our ability to continue as a going concern; uncertainties of cash flows and inability to meet working capital needs; an inability or delay in obtaining required regulatory approvals for Nomacopan (Coversin) and any other product candidates, which may result in unexpected cost expenditures; our ability to obtain orphan drug designation in additional indications; risks inherent in drug development in general; uncertainties in obtaining successful clinical results for Nomacopan (Coversin) and any other product candidates and unexpected costs that may result therefrom; difficulties enrolling patients in our clinical trials; failure to realize any value of Nomacopan (Coversin) and any other product candidates developed and being developed in light of inherent risks and difficulties involved in successfully bringing product candidates to market; inability to develop new product candidates and support existing product candidates; the approval by the FDA and EMA and any other similar foreign regulatory authorities of other competing or superior products brought to market; risks resulting from unforeseen side effects; risk that the market for Nomacopan (Coversin) may not be as large as expected; risks associated with the departure of our former Chief Executive Officers and other executive officers; risks related to material weaknesses in our internal controls over financial reporting and risks relating to the ineffectiveness of our disclosure controls and procedures; risks associated with the SEC investigation; inability to obtain, maintain and enforce patents and other intellectual property rights or the unexpected costs associated with such enforcement or litigation; inability to obtain and maintain commercial manufacturing arrangements with third party manufacturers or establish commercial scale manufacturing capabilities; the inability to timely source adequate supply of our active pharmaceutical ingredients from third party manufacturers on whom the company depends; unexpected cost increases and pricing pressures and risks and other risk factors detailed in our public filings with the
For more information
Investor Contact:
Peter Vozzo
Westwicke Partners
(443) 213-0505
peter.vozzo@westwicke.com
Media Contact:
Mary-Jane Elliott / Sukaina Virji / Nicholas Brown
Consilium Strategic Communications
+44 (0)20 3709 5700
Akari@consilium-comms.com
A photo accompanying this announcement is available at https://www.globenewswire.com/NewsRoom/AttachmentNg/fdb2ed91-9803-4a34-afcd-f1e4c806bff4
![]()
Source: Akari Therapeutics Plc
